Diabetic foot ulcers: treatment, care, and prevention
Diabetic foot ulcers can start small, then become a long and difficult problem if they are missed early. In simple terms, a diabetic foot ulcer is an open sore on the foot that either will not heal or keeps coming back. It often develops where pressure or friction is highest, especially in people with diabetes who have nerve damage, poor circulation, or both.
At Dr KP Meda’s clinic, the focus is on practical diabetic foot ulcer treatment: Finding the cause, reducing pressure, protecting the skin, treating infection if present, and preventing the ulcer from returning. This is especially important because diabetic foot ulcer stages can progress from superficial skin breakdown to deeper tissue involvement and, in severe cases, loss of tissue and amputation.
Before you read on: If you already have an ulcer, or if your foot has any wound that looks new, spreading, smelly, or painful in a way that feels “wrong”, get assessed urgently. Delays matter.
What causes diabetic foot ulcers?
Diabetic foot ulcers typically happen due to a combination of factors. Nerve damage (neuropathy) means the foot loses protective sensation, so small injuries such as blisters, cuts, or pressure points are not noticed. Poor blood flow reduces the ability of tissue to repair itself. Then, infection can move in. Common contributors include:
Neuropathy from diabetes, especially loss of feeling in the feet.
Poor circulation and peripheral arterial disease.
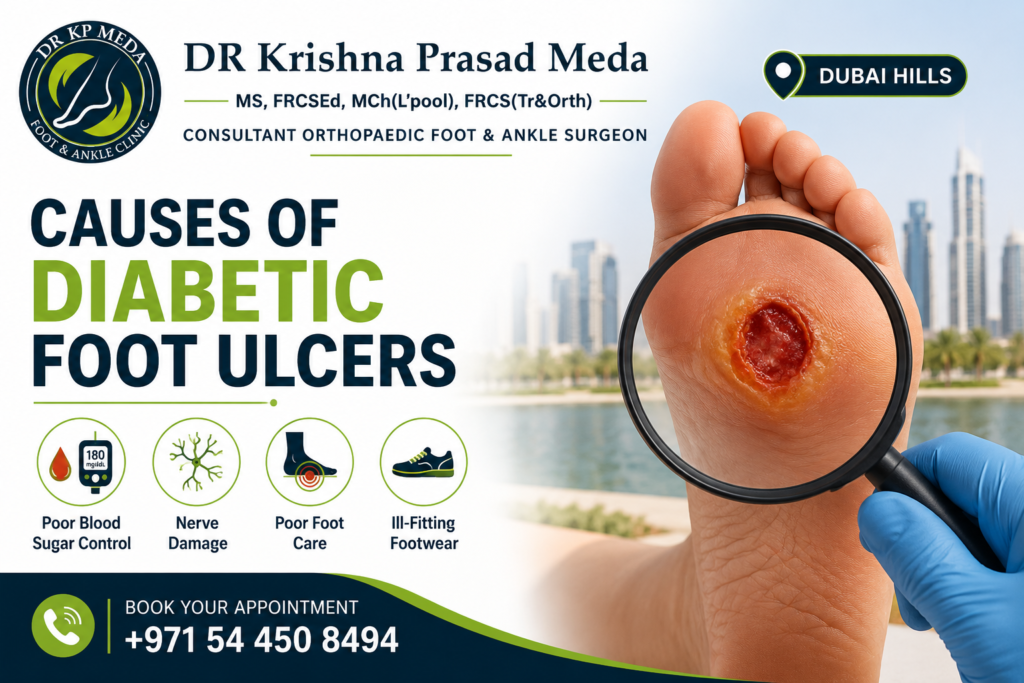
Foot trauma such as rubbing from shoes.
Abnormal toe shape and pressure points, like bunions or hammer toe.
Repeated friction and pressure in one spot.
Previous ulcers or toe deformities that change how you walk
Diabetic foot ulcer stages: what to expect?
Understanding diabetic foot ulcer stages helps people recognise what “early” really means. Ulcers can vary in size and depth. The appearance can also change:
- Yellow, pink, red, grey, black can be seen depending on depth and tissue status.
- Black often suggests dead tissue or gangrene in severe cases.
Stages commonly progress like this:
- Early skin breakdown or a superficial wound.
- Deeper ulcer formation, potentially involving fat, tendon, or bone.
- Signs of infection can appear at any stage, and infections can persist.
- Advanced cases may involve gangrene and tissue loss.
In practice, “stage” is not just a number. It is about how deep it is, whether bone is involved, and whether infection is present.
Complications of diabetic foot ulcer
Complications of diabetic foot ulcer are a key reason treatment must start early. A diabetic foot ulcer can lead to:
Infection spreading to surrounding tissue.
Infection that involves nearby bone, making healing much harder.
Delayed healing and recurrent ulcers.
In severe situations, surgical removal of affected toe or part of the foot.
It is also worth noting that diabetes-related foot problems can lead to hospitalisation when infection or tissue damage becomes complicated.
How to recognise diabetic foot ulcer signs?
Sometimes people do not feel pain because of neuropathy. So the ulcer may be found by sight. You might notice:
Dry or cracked skin
Redness or rashes
A callus over a pressure point that suddenly breaks down
A hard rim or thickened border around the wound
Drainage seen on socks
Brown discolouration
A strong odour
The ulcer getting wider, longer, or deeper over days to weeks
If there is a wound that looks like it is worsening, treat it as urgent.
Diabetic foot ulcer treatment: Assessment and diagnosis
Diabetic foot ulcer treatment starts with assessment. Dr KP Meda works through a structured approach:
Look at the ulcer appearance, edges, and surrounding skin
Note the location, because certain areas correspond to pressure points
Decide whether imaging is needed to check depth and possible bone involvement
Identify whether the ulcer looks neurotrophic (pressure and sensation loss) or arterial (circulation problem)
Tests that may be considered include:
X-ray to check bony involvement
CT scan or MRI to define how deep the ulcer goes and whether it has reached bone
Where relevant, referral to other specialties may occur, such as vascular assessment or surgical planning.
Best treatment for diabetic foot ulcer: Care plan basics
The best treatment for diabetic foot ulcer is not one single thing. It is a combination. And it must match the cause. If the cause cannot be corrected, recurrence is more likely. Treatment usually includes careful skin and foot care plus wound support.
The goal is to heal the wound and reduce pain or pressure. People are different. Lifestyle is different too. Common non-surgical diabetic foot ulcer treatment options include:
- Topical wound care, with keeping the wound covered and moist.
- Antibiotics when infection is present, based on clinical judgement.
- Off-loading to remove pressure from the ulcer area, for example cast, specialised shoe, braces.
- Elevation if swelling is an issue.
- Compression wraps in selected cases as advised by the care team.
- Orthotics and footwear changes to correct pressure points.
- Prosthetics or walking aids if needed while healing.
Surgical diabetic foot ulcer treatment may be needed for advanced or infected ulcers. Examples include:
- Debridement, meaning removal of infected or non-viable tissue.
- Repair procedures for associated deformities, where appropriate.
- Reconstructive options such as skin grafts in selected cases.
- Bone related procedures depending on the site and pathology.
Dr KP Meda is known for a thoughtful approach. Safe surgery only when indicated after reasonable non-operative options have been tried.
Daily diabetic foot ulcer care at home
Home care can make a difference, and it is not complicated, but it must be consistent. Typical advice may include:
Wash the affected area with mild soap.
Keep the wound clean and dry, and change bandages as directed.
Take prescribed medications exactly as directed.
Drink enough fluids and follow a healthy diet advised by the clinician.
Avoid walking barefoot.
Wear appropriate shoes and socks, and use supports or orthotics if prescribed.
It sounds basic. It is basic. But it matters.
Prevention of diabetic foot ulcers: What works in real life?
Diabetic foot ulcer prevention is mostly about routine. Small habits reduce risk over time. The following points align with best practice:
Manage your diabetes and follow your care plan.
Inspect your legs and feet every day, including between toes and on the bottoms of your feet.
Check for blisters, cracks, scratches, redness, ingrown toenails, corns, and calluses.
Use a mirror if needed, or ask someone to check if seeing the area is hard.
Stop smoking if you smoke, and reduce alcohol where applicable.
Keep blood pressure and cholesterol controlled.
Maintain nail care safely, cutting straight across and smoothing edges.
Exercise regularly, under your healthcare plan.
See a podiatrist regularly, especially if you have had a previous ulcer or deformities.
And yes, appropriate footwear is not optional. It is protective.
Who should see a foot and ankle specialist?
If you have diabetes, it is wise to have regular foot checks. Whether or not you have an ulcer right now, earlier assessment can spot problems such as pressure points, deformity-related friction, or circulation issues. Also seek urgent assessment if:
You notice a new wound on your foot or toe.
The ulcer is spreading or draining.
You smell infection.
There is colour change or black tissue.
You feel unwell with fever or the foot becomes hot and red.
Take the first step toward lasting foot health
Don’t wait for a small scratch or a stubborn callus to disrupt your life. Protecting your feet from the complications of diabetes requires timely, expert attention from a specialist who understands your unique needs.
Dr KP Meda at the Foot and Ankle Clinic is dedicated to providing compassionate, advanced care to help you maintain your mobility and safeguard your long-term health.
Whether you need a preventative screening, a personalised nerve sensation evaluation, or specialised wound management, our clinical team is here to support you every step of the way. Take control of your wellness today. Book your comprehensive foot evaluation at the Foot and Ankle Clinic now.
FAQ'S
Diabetic foot ulcers are open sores on the foot that will not heal well or keep returning. In diabetes, nerve damage and circulation problems can cause skin breakdown, sometimes without pain. They can become infected, and in severe cases, lead to surgical removal of affected tissue.
The best treatment for diabetic foot ulcer is a personalised plan based on cause and severity. It often includes wound care, infection management, off-loading to remove pressure, and sometimes debridement or surgery for deeper or infected ulcers. The plan should also address footwear and mechanics to prevent recurrence.
Diabetic foot ulcer stages describe how shallow or deep a wound is and whether it involves deeper tissue such as bone. Stages can also reflect whether gangrene or serious infection is present. Knowing diabetic foot ulcer stages helps with deciding urgency and the right diabetic foot ulcer stages care pathway.
Complications of diabetic foot ulcer include infection that does not resolve, spread into deeper tissues, delayed healing, recurrent ulcers, and severe tissue loss. Advanced cases may require surgical treatment including amputation.
Healing time can vary widely. With proper diabetic foot ulcer treatment, healing may take weeks to months. Ulcers that are deeper, infected, or subject to ongoing pressure can take longer, and some can recur even after healing.
Yes, diabetic foot ulcer prevention is possible and often effective with consistent foot checks, proper
Recent Post

Ankle Pain Causes You Shouldn’t Ignore
Ankle Pain Causes You Shouldn’t Ignore Ankle pain is something many people experience at some point in their lives. Whether it starts after a long

How Do You Get Rid of Plantar Fasciitis?
How Do You Get Rid of Plantar Fasciitis? Heel pain has a surprisingly common culprit. Plantar fasciitis affects millions of people globally every year, making
Diabetic foot ulcers: treatment, care, and prevention
Diabetic foot ulcers: treatment, care, and prevention Diabetic foot ulcers can start small, then become a long and difficult problem if they are missed early.
Symptoms of flat feet: When to see a doctor
Symptoms of flat feet: When to see a doctor Flat feet symptoms are not always a problem. Many people have a low or missing arch
